|
But does it really? I recently sat in on a music appreciation group run by an occupational therapy assistant as a consultant, on an in-patient mental health ward for women. A member of the group started out positively and beamed at everyone; "music makes you happy" extolling the power that it had to lift her mood and to make her feel good no matter how terrible she might have been feeling. Great. I mean, that's really great, no? Some in the room embraced her views with matched enthusiasm. One turned away from her and seemed to retreat inwards towards their own core. I wondered what some music might trigger for her? When I was little my dad used to practice Bach's Preludes and Fugues on the piano that leaned against the other side of the wall to my bedroom. Now that he has been dead for some years this music brings feelings of such comfort and melancholy, all at once, like an embrace from someone you can't quite touch but whose presence you can almost feel. It doesn't just make me happy. It elicits a smorgasbord of emotions all at once, in turn making me need space and time to go into my own head to be able to process this deeply personal and subjective response. Happiness and its pursuit has become big bucks for western society with self-help books, mindfulness apps, bigger, better, shinier appearances and assertion that these things contribute towards a happier self. Music can trigger all kinds of emotional and physiological reactions for people, happiness being just one in the myriad. Retailers play music specially chosen to be the optimum speed, volume and style to induce the consumer to spend more and stay longer. Some tube stations trialled piping in classical music to reduce crime and antisocial behaviour. This example demonstrates that one person's delight can be another person's punishment. At its most extreme, music is used in C.I.A. torture techniques.  Some will say that neither Morrisey or depression are joking matters and I agree. However, it helpfully illustrates the idea that music can make us feel something other than happy. Recently there was a suggestion in a Professional Standards Authority (PSA) consultation - Promoting Professionalism, Reforming Regulation (January 2018) - that some professions cease to be statutorily regulated. This made the various Arts Therapies professions alert to the possibility that we might be among these. It would not have been the first time that others might not have understood the importance of regulation of Arts Therapies, perhaps due to the thought that the arts are warm and fuzzy, creative and happy-making, and could do no harm. These suppositions exist in the minds of many and illustrate a lack of basic understanding for the arts, the arts therapies and for the differences between good practice and dangerous practice in therapy. Misuse or misunderstanding of the arts in a therapeutic setting can cause great harm. Music doesn't just make us happy. Far from it.
Later on in the group session I mentioned before, a piece of music had been chosen and was playing. Someone began to cry. The music was reminding them of something or someone. They didn't want it to be turned off. Another person leaned forward and held their hand as they cried. In reflection together afterwards the message - "music makes you happy" - had transitioned to "music is so powerful". It felt like an important shift for the group and speaks to the core of the matter I'm discussing. Music is powerful and can trigger or support the gamut of human emotional and physiological experiences. It isn't just about making us happy. "Music is part of being human" (Sacks, 2007).
0 Comments
Recent surveying of the music therapy profession in the UK detailed that 38.5% of those who responded had more than one employer, 34% had two or three and 4% had four or more (Carr, C et al 2017). I am one of the 4%. The mental load of the different hats we wear as music therapists can be weighty. A working week containing multiple roles becomes a balancing act with different settings, client groups, admin specifications and venues to consider and hold in mind.
Roles: With the aforementioned in mind, I wondered if it might be interesting to describe an 'average' working week of my own? I currently have six roles, four as a music therapist, one as a Trustee with the BAMT and one co-running Wind Chamber Music Weekends. To focus in on the music therapy ones, I have;
Mondays I start with a half day in one venue. Once I arrive I unpack my instruments. I have managed to work out what I can carry in one journey from the car to the session room which includes a keyboard, guitar and wheeled box of small percussion, hand puppets (don't forget the monsters), plastic farm animals, silk scarves and a parachute (of course!). There is time to make handwritten clinical notes in client's case-files as I go along during the morning . Any other admin, meetings or report writing occur outside of this time. I pack up and head off to my freelance session via the shops where I pick up my lunches for the week ahead. I find that buying ready made lunches on Monday helps to a) eat more healthily and b) remove some of the mental load of planning ahead. When I arrive, I just have time to set up the room, hold the session, support the client in leaving at the end of the session which they struggle with, write handwritten clinical notes and pack up again before heading to the last session of the day. Any other reports or admin take place outside of the time I'm booked for. At the last session I am always greeted at the school by a wonderful member of staff who rushes to hold doors open for me and my bulky load with a warm and welcoming smile. It is incredible what a powerful impact that has on me at the end of each Monday. I smile back and thank her profusely, go to the room, set up, hold the session and pack up again. Notes are written in the car this time as they are electronic. I could do them when I get home but I find that the quality of my note writing is better when they are written as soon after the session as is possible. Also, it means that when I get home and have put away the instruments and transferred the case-files from my locked work bag to the locked cabinet in my office, I don't have anything more to do and if I want/need to, I can put my feet up and unwind. Tuesdays, Thursdays & Fridays These are spent at ELFT in my NHS post. Here I hold 1:1 and group sessions in the adult learning disability service and group sessions in the recovery college. There are meetings, trainings, collaborations, research, managerial and clinical supervision, assessments and much, much more. Everything takes place in the working hours I'm employed for; note writing, reports, supervision and admin. Wednesdays I used to think I had Wednesdays off, and I do sometimes, but in reality they are often the time I use to do the admin from the non-NHS posts, the supervision, the invoicing and the admin from these roles. I also try to fit in the BAMT trustee matters and admin for the music courses... So there we have it. A fairly swift break down of my 'average' week. It all works out fairly well at the moment. Mondays are a well-crafted machine that work well if everything goes as planned but as soon as something goes slightly wrong, such as bad traffic, then the whole machine splutters and then breaks. Wednesdays are usually quite busy despite being labelled as a day off. For me, tricks like buying my lunches on Mondays for the week ahead serve to lighten some of the mental load of having multiple roles. Placing barriers around roles and striving for clear definition of time is also essential. References
What is your job title?
I am an HCPC registered Music Therapist. I currently work with people with dementia and young children with autism. What attracted you to music therapy? I trained as a classical musician but realised after some experiences in my personal life that my interest had shifted to wanting to work with people and to help others. Whilst at music college I took an elective called ‘Introduction to music therapy’ and had my eyes opened to a profession I’d never come across before, one that used music and all its elements as tools to facilitate therapy with people across the spectrum of mental, physical, emotional and social health needs. I discovered that it was first and foremost a therapeutic intervention and a world apart from simply playing music to people to lift their mood. The more I learnt about the psychodynamic and psychoanalytic processes and theories that were inherent in the work, and the different groups of people that it could help, the deeper my interest became. Four years after finishing my undergraduate degree, with some life experience under my belt, I returned to education to study for the two year full time masters that is required in order to qualify and practice. What benefits does it have? Music therapy has its roots deeply grounded in the attachment theories of Daniel Stern, Donald Winnicott and of course, John Bowlby. Mother-infant attachment is non-verbal and as such, the use of music in a therapeutic setting can easily become more understandable. By using the client’s facial expressions, body language and the manner in which they are speaking (combining the words they are using with the way in which they are delivering them; the speed, intonation and volume for example) music therapists are able to get a profound understanding or insight into the client’s inner world. Improvisation and familiar music are used in sessions. Clients are offered instruments and need no prior musical experience or knowledge in how to play them. The way that they play, or choose not to play, offers the therapist insight. The music they generate, no matter how simple or complex, soft or loud, hesitant or confident, is met and supported by the music therapist who uses their own musical response to encourage and enable the client further. Thus, a therapeutic and trusting relationship can begin to grow. For people with dementia who may no longer be able to find the words they seek, being able to communicate through using music in this way can be a lifeline. What is a typical day for you? I work in care homes four days a week, one day in each home, and they are a mixture of residential, nursing, dementia and nursing dementia. On arrival each morning, I speak to the staff team to find out how residents have been in the week since I was last there and then sketch out the day based on this feedback and on my knowledge of who might be most able to have their session at which point in the day. This can be informed by previous patterns, known preferences or health-based reasons and is always subject to change. My hope is to see five people for individual sessions and to hold one large open group each day. Individual sessions are a course of weekly therapy sessions for which people are referred by staff, family, health care professionals or through self-referral. They don’t follow a template or pattern as I work in a person-centred way so each session is tailored to the person that I am working with. Referrals are made for people who may be struggling with symptoms of dementia such as apathy, depression, aggression, frustration or lethargy, to name a few. The focus of music therapy sessions is not to make someone feel happy, but instead it is to try to establish how a person is feeling and to be there with them with those feelings, whatever they might be. Sometimes people are referred due to their love of music but are not in need of therapy and in this instance I encourage them to join us in the open group to make sure their love of music has an avenue. After a six session assessment period, if music therapy seems to be appropriate for a person, I establish therapeutic aims for that person. Some examples of music therapy aims for people with dementia could be:
The open groups can be busy. I think 28 people is the biggest (so far). Due to large numbers, familiar songs are my tool of choice. They offer comfort and structure which in turn provides stability and security for residents who may find the world to be quite a daunting place at times. Residents, staff and visitors are offered small percussion instruments and invited to sing, play or listen, depending on how they are feeling. The most important thing for me is that people are given the encouragement to follow their own wishes, promoting self-determination. Once we start to play and sing it feels as though potential barriers of ability and disability dissolve. The act of making music together seems to stimulate minds and social interactions, and the room is often abuzz by the time we finish, whereas when we started it may have seemed muted and still. What qualities do you think you need to be a music therapist? Being a music therapist requires patience and acute attention to detail. A lot of the work can be noticing the micro-expressions or movements a person makes and responding to them with the same or similar level of intensity. In my work with those who are severely impaired and perhaps are no longer verbal or mobile, these responses to the small movements that they make, or to the pace of their breathing, can offer them a sense of being heard, of being met, of not being alone. Another major quality I think is flexibility and spontaneity. The work is never the same from one day to the next and there are many factors at play in fitting sessions in to the busy life of a care home. What do you find most challenging about being a music therapist? In my work I come across many different people; the older people I work with (clients), their relatives and friends, the staff who care for them and run the homes where they live, my fellow health care professionals and the generous volunteers. With so many people involved it can be tricky to get across what I’m doing, or trying to do for the residents. In the complex jigsaw puzzle of the care system, music therapy is one of the lesser known allied healthcare professions that helps to make up the bigger picture of care. Raising awareness about what music therapy is and how it can help can feel like having a song on repeat; gently correcting and redirecting the well-meant but often mistaken assumptions that people have. What do you like most about your job? It has to be the people and the tools that I work with. Hearing their stories and being able to help them to express themselves when it is perhaps not such an easy thing to do any more is intensely rewarding. Music is something that we can all relate to regardless of age, and is often central to a person’s sense of identity. It provides us with ways to connect and share feelings, memories moments with others, and offers stimulation and encourages expression. I love music and the effect it has on me and on others. Working with music in clinical setting and being witness to the positive changes I can help to bring about due to it continues to surprise and fulfil me. Polly Bowler Polly qualified as a music therapist in 2011 and has worked full time with people with dementia since 2012. She has also worked with adults with learning disabilities and children with autism. She is a trustee for the British Association for Music Therapy and plays for the Bedfordshire Orchestral Society and its two orchestras as well as the Tribe of Tinkers folk collective. Music Therapy & Dementia: Helping Keep Connections AliveBelow is an article I co-wrote with Grace Watts in 2016: As human beings, music plays a fundamental role in our identity, culture, heritage and spiritual beliefs. It is a powerful medium which can affect us all deeply. Playing a musical instrument, being part of a choir or in a band, listening to music – these are all ways in which we can engage in music. They help us to connect with ourselves and others. Music can be exciting or calming, joyful or poignant. It can stir memories and powerfully resonate with our feelings, helping us to express them and communicate with others. Everyone has the ability to respond to music, and music therapy uses this connection to facilitate positive changes in emotional well-being and communication through the engagement in live musical interaction between client and therapist.Oliver Sachs, in his book ‘Musicophilia’, described music therapy as ‘seeking to address the emotions, cognitive powers, thoughts, and memories, the surviving “self” of the patient, to stimulate these and bring them to the fore. It aims to enrich and enlarge existence, to give freedom, stability, organisation and focus. For people living with dementia, music therapy engages healthy parts of the brain to address the secondary effects of the condition, such as loss of confidence and self-worth, low mood and feelings of frustration, irritability and anxiety.  Donald was quiet and almost apologetic of his presence socially. It took him time to find the words that he was looking for and this meant that often, he would not talk rather than putting himself through the trauma of stumbling over words. In his music therapy sessions Donald improvised on the xylophone while the therapist followed the shape and emotional content of his music on the piano. She was able to support and encourage his sense of self and promote his confidence. He commented that he felt “exhilarated” and slowly explained that he found improvising music easier than talking.
Central to how music therapy works is the therapeutic relationship that is established and developed, through engagement in live musical interaction and play between a therapist and client. A wide range of musical styles and instruments can be used, including the voice, and the music is often improvised. Using music in this way enables clients to create their own unique musical language in which to explore and connect with the world and express themselves. For someone living with dementia and for those who care for them, these moments of connection through music can be transformative. Music therapy is a particularly effective clinical intervention for people who have difficulty communicating verbally as musical participation and response does not depend on the ability to speak. For most people living with dementia in the later stages, are able to access memories from long ago, but not recent events. The brain remembers emotional experiences more easily than facts and the emotional nature of music helps these memories come to the fore and helps maintain connections with loved ones and carers. For Donald, isolated by his changing verbal abilities, the realisation that he could communicate his emotions through music to someone who could contain and hold them and that he could create something worthwhile that was his, was a life affirming process. For thirty minutes a week, he was able to communicate with another person without it provoking worry and stress. The sessions moved at his pace, with no musical goals, only the therapeutic aims of enabling him to communicate and express himself in order to help to reduce his anxiety and resultant agitation. Music therapists work with people living with dementia to help maintain their quality of life and care, and look for appropriate ways to use music to help meet their psychological needs. They work with individuals, with families, and in groups. They can offer sessions in a person’s own home, in residential care settings or day centres. Music therapy is an established psychological clinical intervention, which is delivered by HCPC registered music therapists to help people whose lives have been affected by injury, illness or disability through supporting their psychological, emotional, cognitive, physical, communicative and social needs, connect with the world and express themselves. Working in care homes I come across many different people. The older people I work with (clients), their relatives and friends, the staff who care for them and run the homes where they live, my fellow health care professionals and the generous volunteers. With so many people involved it can be tricky to get across what I’m doing, or trying to do, for the residents. In the complex jigsaw puzzle of the care system music therapy is a little piece, a lesser known allied healthcare profession when compared to the role played by carers or GPs for example. Raising awareness about what it is and how it can help can feel like a relentless hamster wheel, gently correcting and redirecting the well-meant but often mistaken assumptions that people have.
So I wondered if I could try to explain some of the common misunderstandings that I have encountered. Bearing in mind that for most music therapists the phrase “so, what is music therapy?” sends shivers down their spine, this could be easier said than done. 1) “It will make you happy” Let’s start here, as to find or to have happiness is a worldwide pursuit. On my way to and from music therapy sessions with residents we are often stopped and greeted. “Have a good time”, “enjoy yourself” and “have fun” are amongst the civilities. In a setting where people are struggling with loss on multiple fronts - loss of identity, loss of occupation, loss of independence, loss of their home and possessions, as well as the losses felt by their relatives and friends - it can become vital for relatives and staff to be able to think of and see the residents being happy. The focus of music therapy sessions is not to make someone feel happy, but instead it is to try to establish how a person is feeling and to be there with them with those feelings, whatever they might be. This is not to say that happiness is not important. It is. But so are all the other emotions that we can experience. People with dementia still feel the full spectrum of emotions that they have always had. However, their ability to cope with or process them may have declined which could lead to frustration, anxiety or agitation. Music therapy can offer a means of non-verbal self-expression, whether the resident is feeling happy or sad, wistful or excited, tired or animated. By using a mixture of improvisation and familiar music the communication of feelings and emotions can be given almost an alternative language. 2) “How did they do?” There is no ‘right’ or ‘wrong’ way for clients to be in sessions. They cannot get it ‘wrong’ as sessions are person-centred and the therapist follows and supports them in whatever mood or state they are in. So I suppose the answer to this will always be that they did it perfectly. I sometimes wonder if this also ties into a mistaken belief that I am there to teach the residents. Perhaps this is because music lessons are a more familiar concept than music therapy so people jump to that to answer what I do in their minds? The irony is that I am an instrumental music teacher. I have taught cello, sax and piano for years. But the two professions are worlds apart. 3) “You wouldn’t want to see them!” …”they’re too challenging.” Staff can sometimes seem to be trying to protect me from the challenging behaviours that residents can exhibit as a result of their confusion/dementia. Often, these are the very behaviours that I am trained and employed to try to help the resident and home with. Challenging behaviours can be anything from wandering or perambulating, to physical aggression and the whole spectrum in between. Imagine having a surge of emotion but not being able to understand what it is yourself, and also not being able to communicate it to anyone else. By the therapist’s intense observations of body language, facial expressions, tone of voice and any verbal interaction offered they can try to gauge how someone is feeling and to then meet them with music to support and validate those feelings. This can lead to the resident feeling responded to and understood which in turn can lead to their mood changing. But if it doesn’t change that is ok too, and we can remain in their current emotional state together rather than them being there alone and unsupported. 4) “Why don’t you see so-and-so instead?” What is the saying about best laid plans? Seeing people for sessions in the place that they live in means that there can be a vast number of things that can prevent you from being able to have a session when you had hoped. The resident might not be up yet, or they might be doing something else or demonstrating their right to choose by not coming (it is important to respect people’s autonomy). Consequently, the usual boundaries of time and place associated with therapy may need to become flexible in order to facilitate sessions. I work with individuals who have been referred to individual music therapy for weekly sessions. The referral process at my workplace (it will be different in other establishments) enables me to learn about the resident’s personal history, their medical diagnosis, the medication/s that they are prescribed and the potential side effects that they could cause, possible risks both to them or to me, the reason that the referral has been made and so on. After referral, six assessment sessions are offered. This process enables a more thorough understanding of the resident as well as the chance to establish therapeutic aims for the course of sessions. Seeing people for one-off sessions can be done, but it is a very different process without this background knowledge. That isn’t to say it is better or worse, just different. It is my priority to try to see the residents who have been referred to me and are ‘in therapy’. 5) “Are you doing music entertainment later?” I run an open group therapy session each day. The term ‘open group’ means that anyone can come or go as they please. I’ve mentioned the confusion that people with dementia can experience. This, combined with the common hearing problems that older people can have and the difficulties with processing situations or events occurring around them, can make it problematic to run large open groups in the traditional improvisation-based manner. The structure and familiarity offered by pre-composed, well-known songs and tunes can provide residents with a feeling of relaxedness and comfort. This in turn can provide a foundation for increasing positive social interactions and communication between the members of the group. Isolation is a common result of dementia. Depression can be a common secondary symptom too, which itself can lead to isolation, lethargy and apathy. Engaging residents with familiar music can promote opportunities for sociable encounters with others. And once people are engaging and interacting it can be possible to encourage improvisation. This promotes spontaneity and creativity which in turn can raise self-esteem and feelings of being skilled. And finally… There are many more misconceptions surrounding music therapy, but more importantly there is a growing understanding of our clinical work. As staff see their residents respond to both the individual and group sessions they themselves become more interested and supportive of sessions, enabling residents to attend and offering them gentle encouragement if they seem unsure. We are able to work as a multi-disciplinary team, feeding back important observations and suggestions to each other. As music therapy reaches and helps more clients and their families, people’s understanding of it will continue grow. Dementia affects an ever growing number of people and it affects each of them differently. Music therapy offers a person centred, non-drug based intervention which can be relevant in the early stages of dementia all the way through to end of life care; for those at home in the community, in hospital or in care homes, regardless of the challenges and difficulties that the client might be experiencing. As a profession we strive to continue to learn and keep our knowledge up to date in order to best meet the individual needs of our clients. No two sessions are alike, just as no two clients are the same. Our training enables us to tailor sessions to the ever changing needs of the individual. It is both a challenge and a privilege to carry out this work. I work with elderly people with dementia in care homes run by Methodist Homes. I recently came across a case which troubled me and caused me to search related literature for similar instances. I was hoping to find advice, protocols and ideas as to how to assist and work with people going through this experience, but I discovered that there is very little research on the topic in both the music therapy and wider literature. The topic that I was researching was grief and dementia. I came across countless papers and articles covering the grief of a caregiver, spouse or other close family members when a person with dementia dies, but very few on the grief of a person with dementia when their spouse or family member dies, which is what I was witnessing first hand. The papers that I found were not music therapy based but were from other health care professions’ journals such as The American Journal of Hospice & Palliative Medicine and The Journal of Geriatric Psychiatry and Neurology.
My case involves a married couple who were living in the same care home, both with dementia and both still happy and in love. The husband died unexpectedly and now his wife is struggling to understand what has happened. Each day brings a different presentation. Some days she doesn’t remember what has happened and enters in to in a cycle of agitatedly asking where he is, facing the constant re-traumatisation of learning that he is dead and then denial as she shouts at staff, accusing them of lying, and goes off in search of him. Some days she is aware and seems to be able to grieve in a more accepting manner. Other days she wanders the unit looking for him although without the urgency or aggression shown previously. I have had one assessment session with this lady. She was wandering the unit constantly, looking for her husband. She was not agitated or aggressive but had a look of quiet determination about her. I invited her in to my room and we talked. I asked her about her husband, as I remembered reading about successful therapeutic interventions such as sharing favourite memories of the deceased and the life they lived (Gataric, Kinsel, Currie, & Lawhorne, 2010). I carefully spoke of him in the past tense and she did not correct me. She spoke of him in the present tense and I did not correct her. We spent 30 minutes together starting in the music therapy room, moving to her bedroom and finishing in the dining area. Her desire to find her husband made it necessary to travel with her in order to be able to spend any time with her. This was a significant interaction as other staff had reported that they were finding it difficult to spend any length of time with her without her mood becoming heightened and anxious. I found that in the 10 minutes that we spent in the therapy room I was unable to introduce music of any kind. Initially I thought this was because it did not feel appropriate but on reflection I wonder what else might have stopped me. My own emotional response to her situation was profound. I struggled not to become overwhelmed by the depth of my feelings elicited by her loss and her inability to process what had happened. I wonder; if this could have blurred the boundaries between us; how to try to get past this if it is the case; how to begin to incorporate music in to the sessions? My initial search through the literature seemed to reflect a lack of research in the area of Grief and Dementia. It has also highlighted other cases in my caseload that relate to the topic such as anticipatory grief for the husband where his wife has severe dementia, stage 7 in the global deterioration scale (Resiberg, Ferris, de Leon, & Crook, 1982) and a lady whose husband has died but her family have chosen to not keep reminding her of the loss. “The choice of whether to lie to a loved one or re-traumatise her is no choice at all; both can have devastating emotional consequences.” (Grief & Myran, 2006). I find myself still seeking guidance and other experiences in this area of dementia work. Supervision and peer supervision will be invaluable. If anyone has come across a similar case or any relevant reading that might help me please get in touch using the comments. Bibliography Gataric, G., Kinsel, B., Currie, B. G., & Lawhorne, L. W. (2010). Reflections on the Under-Researched Topic of Grief in Persons With Dementia: A Report From a Symposium on Grief and Dementia. American Journal of Hospice & Palliative Medicine / Vol. 27, No. 8, 567-574. Grief, C. J., & Myran, D. D. (2006). Bereavement in Cognitively Impaired Older Adults: Case Series and Clinical Considerations. Journal of Geriatric Psychiatry and Neurology / Vol. 19, No. 4, 209-215. Resiberg, B., Ferris, S. H., de Leon, M. J., & Crook, T. (1982). The global deterioration scale for assessment of primary degenerative dementia. American Journal of Psychiatry, 1136-1139. In March/April 2013 at my place of work our music therapy team began to develop new feedback forms to use following music therapy open group sessions. The open groups can often be large with numbers sometimes reaching 20 or more as participants, family, friends and staff attend. The forms were to record participant's changing mood, level of participation, use of instruments, musical interaction, non-musical interaction etc using a mixture of quantitative and qualitative data collection. The nature of the large groups led me to feel that a simple and fast method of making a record of the obvious and primary interactions taking place in the group was required and so I developed the Shell Matrix. I offered it to the music therapy team at work and we have been trialling it alongside the feedback form over the past few months. The concept is to be able to record a general impression of the group quickly and easily following the session taking place. This will hopefully provide a memory aid for more detailed notes as well as being a visual representation of the main dynamics and interactions of participants. There is scope for the matrix to be developed further utilising more symbols/keys to represent more detailed interactions as well as the idea of creating more than one per group in order to detail the process through the group. I hope to explore these options imminently but first felt a need to document the original concept. How it works: Participants are represented by small circles in a rough estimation of where they sat in the room. Names can be used if it is appropriate with the rules of confidentiality of the individual setting in question. In the following examples participants are represented by letters of the alphabet. The therapist is placed at the bottom of the matrix (remembering that this is a depiction of the entire group in one matrix so may not have enough detail to be able to document the different positions that the therapist was in). 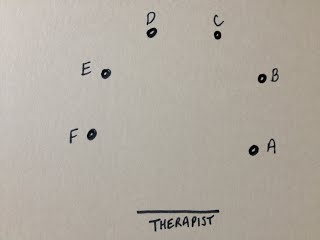 Interactions are illustrated with lines. Straight lines for "good" interactions and zig-zags for "bad". The following example indicates that participant F interacted well with the therapist but that participant F & E did not interact well with one another. However, participant E interacted well with the therapist and with participant D, who also interacted well with the therapist. 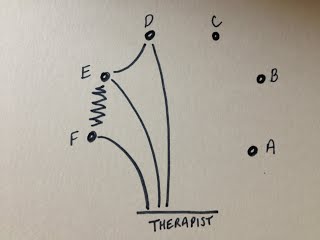 If a participant did not interact at all the two small lines are used. If they did not interact but were still seemingly observing or listening then one small line is used. The following example indicates that participant C did not interact with peers or therapist but could have been observing or listening. Participant A might have been asleep.  To complete the matrix we need to establish participant B's interaction. The following example indicates that participant B interacted well with the therapist and with participant D. 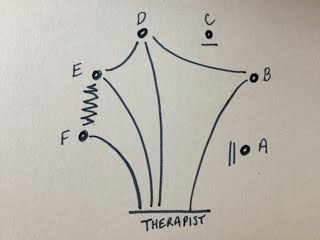 Why the name - Shell Matrix? If the participants all interacted well with the therapist and also with the participant sitting next to them then this is the result... 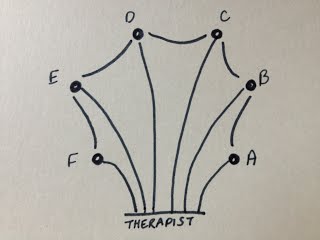 It reminded me of a scallop shell, hence the name. The examples above are simple versions of a simple device. There are many ways that this matrix can be used and other notations that can be used which I will detail soon.
|
AuthorPolly qualified as a music therapist in 2011. In this blog she speaks about music therapy and other related musings. Archives
April 2019
Categories |
 RSS Feed
RSS Feed
